Addressing psychological morbidity in informal carers at the end of life: evidence synthesis and stakeholder consultation to produce tailored, evidence-based information and priorities
What did we do?
This research project aimed to reduce psychological morbidity amongst carers of people at end of life, through:
- evidence-synthesis of factors that affected the psychological morbidity of carers of people at end of life;
- the translation of synthesised findings into accessible, tailored information for key stakeholders to support targeted efforts to reduce carer psychological morbidity and its impacts.
Why was it important?
Some 500,000 UK informal carers provide substantial care and support to people who are nearing end of life, and they may spend an average of 70 hours a week on caregiving in the final months.
This can take its toll on carers' psychological health, with 83% of carers suffering high levels of clinically significant psychological morbidity during the patient's final three months; most carers suffer anxiety, depression and stress at levels that give cause for concern.
We know that both external and internal factors affect carers' likelihood of developing psychological morbidity; many of these could addressed by providing targeted, earlier support to those most likely to develop psychological morbidity.
However, evidence relating to these factors had not been synthesised, and did not exist in an accessible format for key stakeholders.
This reseach project provides the first comprehensive evidence synthesis of the factors that affect the psychological morbidity of carers.
How did we do it?
WP 1 (Month 1-15): Comprehensive mixed-method literature review and synthesis
We undertook:
- reviews of quantitative observational studies using box score and meta-analyses,
- reviews of qualitative studies using a thematic best-fit framework synthesis approach, and
- reviews of interventions using pooled effect sizes and sub-group analyses.
We also integrated the review findings into a framework, which was informed by stress models and carer perspectives.
Carer advisors and a carer co-analyst helped to inform the search strategy, qualitative thematic analysis and framework construction to ensure that our outputs were relevant and accessible to carers.
WP2 (Month 9-18) Stakeholder involvement
- We consulted with a wide range of stakeholders to support the translation of the findings from the literertaure reviews and syntheses (from work package 1) to create bespoke information, priorities and procedures.
- We held a workshop with policy makers, commissioners, researchers, practitioners, and carer representatives to assess the relevance of the findings to their respective spheres of influence (settings and systems), allowing us to identify the most important information and priorities.
- We worked with our review advisory panel to develop a range of targetted dissemination outputs and strategies (see findings and downloadable resources sections below for more information).
- We held a focus groups with practitioners and carers to explore how the project outputs could be operationalised into primary and community care procedures.
Findings
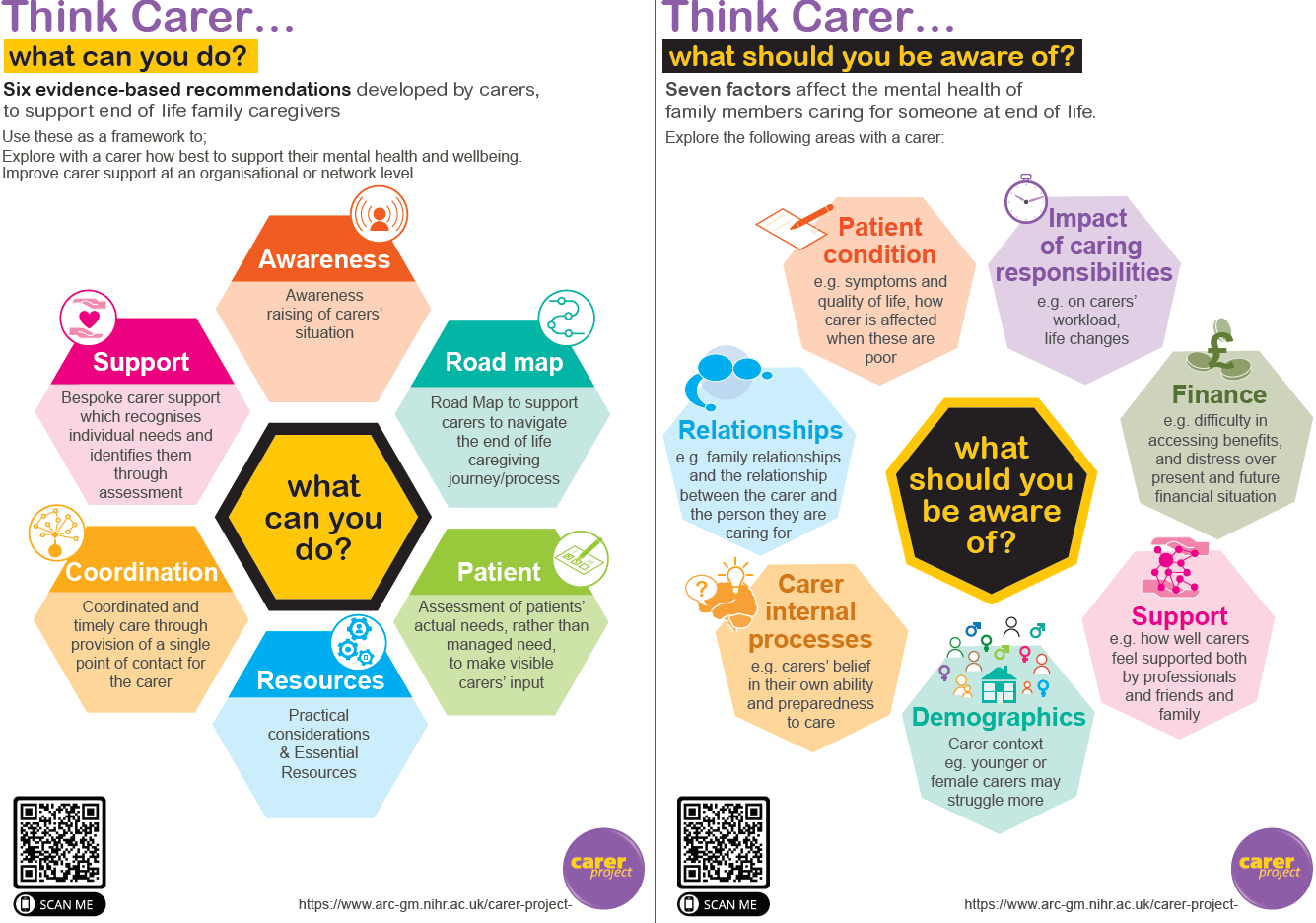
From the systematic reviews and thematic syntheses of a) observational quantative studies, b) qualitative studies and c) a meta synthesis of the literature, we found there to be seven emergent themes (or factors) that had either positive or negative effects on carers' mental health:
- Patient condition: worse patient psychological symptoms and quality of life were generally associated with worse carer mental health. Patient depression was associated with higher depression in carers. Patients’ other symptoms and functional impairment may relate to carer mental health, but findings were unclear.
- Impact of caring responsibilities: impact on carers’ lives, task difficulty and general burden had clear associations with worse carer mental health.
- Relationships: family dynamics and the quality of the carer–patient relationship may be important for carer mental health and are worthy of further investigation.
- Finances: insufficient resources may relate to carers’ mental health and warrant further study.
- Carers’ psychological processes: self-efficacy and preparedness were related to better mental health. However, findings regarding coping strategies were mixed.
- Support: informal support given by family and friends may relate to better carer mental health, but evidence on formal support is limited. Having unmet needs was related to worse mental health, while satisfaction with care was related to better mental health.
- Contextual factors: older age was generally associated with better carer mental health and being female was associated with worse mental health.
You can also watch this video by Dr Tracey Shield, who talked about some of the early findings in her "Evidence synthesis of factors affecting family carers' psychological wellbeing" presentation at the 17th European Association for Palliative Care (EAPC) World Congress 2021.
The full findings from all three of the systematic reviews are available in the 'downloadable resources' below.
Research team
- Prof. Gunn Grande (Principle Investigator)
- Dr Catherine Millington-Sanders (Co-investigator)
- Dr Christine Rowland (Co-investigator)
- Dr Maria Panagioti (Co-investigator)
- Prof. Alison Wearden (Co-investigator)
- Prof. Morag-Farquhar (Co-investigator)
- Prof. Penny Bee (Co-investigator)
- Mrs Sharon Aldridge-Bent (Co-investigator)
- Ms Jackie Flynn (Public contributor)
- Miss Danielle Harris
- Dr Alexander Hodkinson
- Dr Tracey Shield
- Dr Gavin Daker-White
Who we worked with:
The research team worked closely with members of the public who had experienced end of life caregiving to:
- develop the research project and secure funding,
- help us make sense of the information we find
- co-produce summaries of information for people to use in the future
- work with us to get the information out to the people who might find it useful
We are also worked with various professional people throughout the project, in particular we worked with professional stakeholders to develop and tailor information summaries to the numeorus stakeholder groups that support carers.
Downloadable resources
- Publications and reports
- Carer recommendations
- Think Carer - Posters and leaflets
- Information guidance and tables
Levels of information - overview
Level 1 - Broad overview of the evidence
- Pictorial guide of overarching themes and factors related to carer mental health
- Pictorial guide to the information
Level 2 - Detailed overview of the evidence
Level 3 - Quantitative Research Evidence: In-depth summary of factors affecting caregiver mental health overall
Level 4 - Quantitative Intervention research information: in-depth list of factors associated with different types of mental health outcomes
- Protocol
- Carer Project Podcast Series
Series overview.
In this short series of podcasts, members of the research team discuss what we learnt from the carer project about what may worsen or improve the psychological health of unpaid carers for people at end of life. Each episode covers findings within a specific theme or set of themes. The final episode discusses the carer recommendations which were created from the findings by the project’s carer Review Advisory Panel.
The series is hosted by Dr Christine Rowland and Professor Gunn Grande, with contributions from Dr Tracy Shield, Ms Danielle Harris, Professor Alison Wearden, and Mrs Jackie Flynn (Chair of the carer Review Advisory Panel).
Episode 1: Patient Condition. In this episode researchers Christine, Gunn, Tracey, and Danielle explore how carers’ mental health is related to patients’ condition.
Episode 2: Caregiving, relationships and finance. Episode two covers three themes - how carers’ mental health is related to caregiving impact, quality of relationships and finance. In this episode Christine and Gunn are joined by Tracey and Danielle
Episode 3: Internal processes. The topic of this episode is how carers’ mental health is related to their internal processes, or, how they think and feel about themselves. With researchers Christine, Gunn and Tracey
Episode 4: Support. In episode four, Christine and Gunn are joined by Alison to discuss how carers’ mental health is related to the support received.
Episode 5: Contextual factors. How contextual factors are related to carers’ mental health is discussed by researchers Christine, Gunn and Alison
Episode 6: Carer recommendations. Recommendations on how to support carers were developed by the project’s carer Review Advisory Panel (RAP) and are discussed in this episode. RAP Chair Jackie joins Christine, Gunn and Tracey.
{kind=link}
Blogs & Presentations
- An introduction by Prof Gunn Grande
 Hello, my name is Prof Gunn Grande and I lead this project. I’m originally from Norway and have lived and worked in the UK for over 30 years.
Hello, my name is Prof Gunn Grande and I lead this project. I’m originally from Norway and have lived and worked in the UK for over 30 years.My work focuses on the central role that family members play in supporting people towards the end of life. Families, and sometimes friends, give vital day-to-day emotional and practical support, helping to make care at home possible. Giving help and care to someone at end of life can put family members under a lot of stress. It is really important to support the family if we are to support the person who is ill.
During the COVID-19 crisis, we have been relying even more on care given by families because it has been more difficult for nurses and other staff to visit people’s houses to help.
The aim of this project is to help family members stay in good mental health whilst caregiving. To do this, we need to understand what can help them cope and what may make things worse.
There has been a lot of research in the past looking into what can make family caregivers’ mental health better or worse. This information has never been pulled together into one place and hasn’t reached those who can make best use of it. In this project we want to change this! We want to pull all the information together and then share it with family members and people who help support family members, such as doctors and nurses, those who plan and fund services, and carer organisations. We will ask people from these groups to help us find the most important messages from the information we gather, and then help us present them in ways that they feel will be most useful.
We are already working with a great team of family caregivers who are advising us on every stage of the project. Some of them are writing blogs for us too, so watch out for those! In the next months we will also bring members from other groups on board to tell us what they think.
The COVID-19 pandemic has definitely made some parts of the project more challenging! But, it has also made us even more aware of just how important it is to support family members who are looking after someone who is ill. This has given us a lot of motivation to meet the challenges COVID-19 has brought! It feels more important than ever to make sure the right information is out there so that family carers can get the best support possible.
- A carer's view by Margaret Booth
 In this blog we hear from one of the members of our carer Research Advisory Panel, Margaret. Margaret describes why and how she got involved in the project, and what working on the project has been like for her …
In this blog we hear from one of the members of our carer Research Advisory Panel, Margaret. Margaret describes why and how she got involved in the project, and what working on the project has been like for her …I was told about this project by a member of the Dementia Carers Expert Reference Group which was advising Dementia United a project to improve dementia care in Greater Manchester. https://dementia-united.org.uk. I thought I might have something to contribute as I cared for my aunt who died of dementia in 2018.
I knew that palliative care for people with dementia who stayed at home was difficult to get. We were “lucky” in that my aunt also had a diagnosis of well controlled cancer. We eventually contacted MacMillan Cancer Support to find that despite the title of the organisation they also provide end of life care for all conditions. Since that time I have been very keen to try to get and share information about end of life care for dementia. I feel that most research on palliative care is restricted to cancer and a few other specific illnesses and more consideration could be given to chronic diseases in the end phase.
I had to fill in a form to apply to be on the project, and I was a bit late. The forms were in Microsoft Word which I hate but I managed it eventually. I am getting much better at using Microsoft now. We also get printouts of all the documents we will need for each meeting posted to us in good time. So even if I can’t find my way round Word I’m OK.
I was very pleased to be able to join the panel and found the first meeting at Manchester University was very well organised. The research team were very welcoming and we actually did get a free lunch. We were told what the project was about and what we would do at the next meeting and we all left very cheerfully. Then COVID-19 took over all our lives. The meetings moved smoothly onto Zoom with a slight detour around something called Doddle that didn’t make the final cut.
We have been kept up to date with the work that the researchers are doing and it is clearly a lot of work. I am very pleased to be involved however slightly with a project that has continued through this pandemic. I know that other organisations have had to restrict or stop their work. It’s reassuring to be part of something is continuing in more or less the way it was planned to.
The researchers have so far been collecting and looking at what data is available and we have had regular updates on their progress at whittling it down to a manageable size. It’s been very interesting to hear what they say.
The Zoom meetings are going quite well. I did ask if they could be shortened a little as I find concentrating on Zoom for three hours difficult. I have slightly weird eyesight and my eyes tire easily. There was absolutely no problems about it, we now have shorter meetings. I feel that everyone gets to have their say which is quite an achievement on Zoom. I would of course prefer to meet face to face and hope we might again before the project is finished. I know that I do tend to talk too much and it’s hard to tell on Zoom when you are boring someone - or everyone. On the other hand you don’t have to venture out in the rain or snow.
I am glad we got to meet each other before lockdown. I think it would have been much more difficult to gel as a group if we hadn’t had that initial meeting, but perhaps we would have been ok.
As a former carer I am determined try to make life easier for current carers because I remember that when you are in the thick of it you just don’t have the time and certainly not the energy to argue your point.
I am fortunate in these chaotic times to be part of something that is working, and even more pleased that it is something that I care about deeply.
- The role of a researcher and what on earth is 'evidence synthesis' by Dr Tracey Shield
I’ve been asked by our team to explain a little bit more about what is involved in this project and what my role is.
I’m a research fellow and that means that I take day-to-day responsibility for making sure the project runs smoothly. My main role is to carry out the research itself – more about that later – and to work with our Research Advisory Panel to make sure what we are doing makes sense to carers and ‘feels right’.
As the research tasks come to an end, I’ll be writing up our findings so we can publish them. I will also be working closely with stakeholders during workshops to produce useful summaries of what we find.
There are two parts to this project.- The first is a big review of current evidence about carer outcomes. However, there’s a huge amount of evidence! It my job to help find all the evidence and then to synthesise it. When I say synthesise what I mean is breaking all the evidence down into easy to manage chunks of information. Then we can sort these chunks into different categories and think about it that way. For example, some of the categories might be: ‘things that predict anxiety’, or ‘things that predict depression’. By doing it like this, it makes the large amounts of evidence we find more manageable and easier to think about. At the end of all of this ‘synthesis’ we can see more clearly the ways people can be affected by their caregiving role. Most importantly, it also gives us an idea of different ways we might be able to help carers.
- The second part of this project includes working with carers with experience of end of life caring. We work with carers themselves to get their perspective on whether the evidence we find and the conclusions we make are meaningful to them. We ask them if what we’ve found sounds like their experiences or not, and makes sense to them. We also ask them if they think there’s anything missing from the evidence we find? What is special about this project is that the carers we are working with are helping us to organise the project findings into different formats. We are doing this so that lots of different people, like health care providers or policy makers, can more easily understand our findings as they are the type of people who can use the information to better support carers.
So, you can probably see that this is quite a big project.
Please do get in touch if you'd like to know more about this research.
- Supporting carers’ mental health. Synthesis of research on factors affecting family carers’ psychological wellbeing
Gunn Grande, University of Manchester
Conference: Seth’s Legacy: Seeing & Supporting People in Palliative & End of Life Care. Hosted by University of Liverpool School of Medicine & Liverpool UHFT.
Organised by Lesley Goodburn.
Funding information
This study/project is funded by the National Institute for Health and Care Research (NIHR) Health and Social Care Delivery Research Programme (HS&DR), Award ID: 18/01/01
The views expressed are those of the author and not necessarily those of the NIHR or the Department of Health and Social Care.
Contact information

Programme Manager
Alison Littlewood
alison.j.littlewood@manchester.ac.uk